Migration Health Evidence Portal for COVID-19

This evidence portal is a repository of research publications and high-yield evidence briefs on COVID-19 and its intersection with migration health.
The scientific literature and knowledge base on the epidemic rapidly expand daily. Tremendous efforts are being made by the global community of clinicians, researchers, and journal editors to advance scientific evidence to guide policy and decision-making at the field level. There is a need to build evidence platforms for sharing and distilling key findings emergent from the growing body of scientific literature, relevant to migration, health, and human mobility. These findings can ultimately assist evidence-informed decision-making from a migration lens.
The portal contains:
-
An interactive, open-source, searchable (and downloadable) repository of research publications on COVID-19 in relation to migrants, migration, and human mobility based on the quantitative analysis of the thematic trends and impact of relevant publications.
-
The full paper of the quantitative analysis of publications on COVID-19 and migration health (i.e., bibliometric analysis), which is regularly updated to include the latest peer-reviewed studies available.
-
High-yield evidence briefs that align with the COVID-19 Global Preparedness and Response Plan and with IOM’s Global Strategic Preparedness and Response Plan (SRP).
-
Profiling migration health and COVID-19 related analysis, research, and commentaries in partnership with the Migration Health and Development Research Initiative (MHADRI), a global network of migration health research experts/scholars.
Research Publications on COVID-19 and Migration Health (covering the period: 01 January 2020 to 31 December 2020)
This section reflects the output of the publication mapping exercise (i.e., bibliometric analysis) involving the quantitative assessment of a set of published scientific articles on COVID-19 with reference to migrants, migration, and human mobility. Bibliometric analysis provides an important snapshot of a specific field of interest/domain. The baseline information from bibliometric analysis helps identify research gaps that future studies can investigate. The analysis enables examining the relevant literature in terms of its scope and content, data use, representation of specific research areas, or its development over time. The bibliometric analysis conducted by IOM and MHADRI on international migration and health is one example.
Key messages
-
Overview of search: The search strategy retrieved a total of 1,953 publications relevant to COVID-19 and migration health, covering the period, 01 January 2020 to 31 December 2020. Many of the publications were research articles (59.9%) and mostly covered the following subject areas: medicine (61.0%), social sciences (21.1%), and environmental science (7.6%).
-
Research themes: The publications relevant to migration health and human mobility mapped by research themes included: public health interventions (42.7%), disease epidemiology and mathematical modelling (28.2%), impact assessment and policy analysis (17.5%), health system capacity (10.0%), migrant specific themes (9.5%), and clinical management (8.3%). Research themes such as: diagnostic and testing strategies, and candidate therapeutics and vaccines were largely under-represented in the current evidence base (less than 5 per cent of the 1,953 publications). About 10% (n=190) of the publications used mathematical modelling to predict spread, and model social distancing, border closures, and impacts on the health care system capacities. Of this number, about 28 per cent (54 out of 190) were global in scope and about 25 per cent (48 out of 190) covered China. There were only two studies that investigated situations in camps settings. These findings highlight the importance of considering the migrant- and migration-health-related concepts in research and scientific communications.
-
Migrant groups and mobile populations: Most studies investigated cases of COVID-19 in the context of population movement. Approximately 22 per cent (n=426) of the retrieved publications mentioned or referred to a ‘migrant’ in the title or abstract A few publications covered specific migrant populations: migrant workers (33.1%, n=141), immigrants (26.1%, n=111), returning migrants (6.8%, n=29), undocumented migrants (6.6%, n=28), migrants in detention (3.5%, n=15), irregular migrants (0.5%, n=2), and migrant families, dependents, and children (n=10). Over one-fourth (n=521) of the publications covered non-specific mobile populations (i.e., tourists and travelers) with majority covering public health interventions and disease epidemiology.
-
Refugees, asylum seekers, and displaced populations: Most of the publications involving refugees (n=112), asylum seekers (n=44), displaced population (n=32) were mainly on protection support services in the health response against COVID-19.. Further, these publications discussed in length the risks and pre-existing vulnerabilities (i.e. overcrowded and poor living conditions, multiple barriers to health care, and others), and the humanitarian barriers that refugees face due to the mobility restrictions implemented by the governments [1, 2, 3, 4, 5, 6].
-
International students: On publications that covered international students, a little over half covered public health interventions (n=24, 53% out of 45), and half of these publications discussed the impact of COVID-19 on the mental health of Chinese students abroad (n=12).
-
Migrant workers: There were about seven per cent publications (n=141) retrieved from the search that specifically involved migrant workers. On themes, about 77 per cent covered impact assessment and policy analysis, and public health intervention. A closer look found that majority of the publications covered India (n=33, 23.4%), wherein public health measures (n=19) mostly refer to mental health and psychosocial support, travel and social distancing measures.
-
Ethnic minorities: This mapping exercise retrieved 36 (1.8%) publications with the keyword ‘ethnic’, referring to ethnic minorities alongside migrants as a high-risk group. However, it should be noted that the methodology of this mapping exercise was not designed to capture ‘ethnic minorities’. Beyond the search results, a relevant systematic review emphasized the importance of gathering robust evidence on the role of ethnicity in COVID-19 [7]. From the said review, several publications in the UK and the US indicated the disproportionate risk of having COVID-19 and suffering from more serious clinical outcomes (e.g. hospitalization, intensive care admission, and deaths) among individuals from Black, Asian, and Minority Ethnic (BAME) groups relative to White patients. Although ethnicity is different from migrant status, the disparities in health outcomes of specific ethnic minority groups may provide a better understanding of the intersection between migrant status and ethnicity.
-
Patient mobility: They were eight publications that discussed ‘patient mobility’ which refers to the national and international movement of patients. Five of the publications covered aeromedical transportation of suspected and known COVID-19 patients across international borders [8, 9, 10, 11, 12]. Two publications discussed interhospital transportation of patients by land and air [13, 14]. One publication noted concerns on the burden of international travel restrictions for coronary heart disease patients from low- and middle-income countries (LMIC), either subsidized by governments or philanthropic bodies. It stressed that reintroducing health care services during and after the COVID-19 pandemic will have to consider the major backlog of surgical procedures in countries that rely on sending patients abroad [15].
-
Most active countries: Most publications involved studies conducted in the US (24.5%) and China (16.4%) suggesting the limited coverage of relevant research in other countries. The top three active institutions identified were London School of Hygiene and Tropical Medicine, The University of Hong Kong, and Harvard Medical School. Africa, South America and the Caribbean, and the Middle East were the least productive countries in terms of the number of research outputs.
-
Research collaborations: International research collaboration was strongest between the US and UK, followed by the US and China, and the UK and China. Details on collaboration networks may be useful in developing multi-center research studies when more robust data become available.
-
There is limited inclusion of migrant status within data collection practices in routine health information systems, hospital registries, and disease surveillance systems globally. This also extends to research where migrant status remains poorly captured. Data disaggregation by migrant flows and categories on COVID-19 testing, hospitalizations, and deaths by migrant status is a poorly described national data set.
-
Conclusions: Efforts to address the challenges of COVID-19 in the context of migration health requires a robust knowledge base generated from the growing body of scientific evidence that carefully considers specific dimensions of COVID-19 and migration health. Although limited to the analysis of relevant publications using the metrics available (i.e. number of publications, co-occurrence of keywords, etc.) the key findings from the analysis can provide a useful starting point that can facilitate ongoing and future research on COVID-19 and migration health in terms of the critical areas that need more attention.
Network map of common keywords
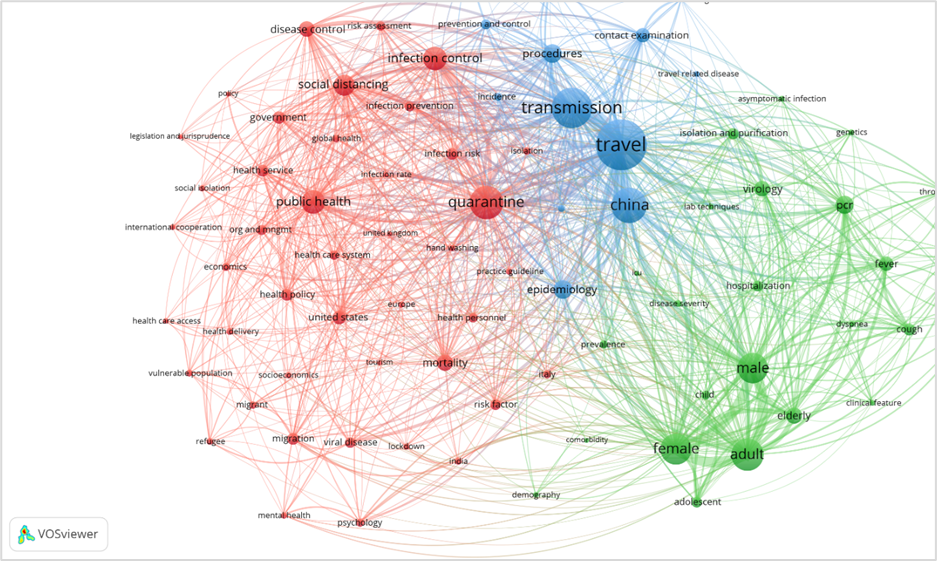
The network map below shows an overview of the common keywords that appear in the title, abstract, and keywords of the relevant publications retrieved on the topic of COVID-19 and migration health. Network maps of keywords reveal key topics in a research area or domain as well as the relationship (co-occurrence) between common keywords. It is a relative indicator of important research areas that are drawing attention in the field. The relationships described are based on the co-occurrence of keywords in publications and do not necessarily represent a structured conceptual framework. Nevertheless, it can provide insight into the extent of the representation of themes on COVID-19 and migration health.
-
The large circles in the figure represent the most frequently occurring keywords in the publications retrieved (N=1,953). The most commonly encountered keywords were: travel’ (n=563), ‘transmission’ (n=446), ‘China’ (n=395), ‘quarantine’ (n=374), ‘adult’ (n=359), ‘female’ (n=346), ‘male’ (n=342), ‘infection control’ (n=265), ‘public health’ (n=261), and ‘social distancing’ (n=239).
-
Using a minimum occurrence threshold of 55 (i.e., each keyword appears at least 55 times in the dataset to be included in the map), the visualization of keywords in the retrieved publications included 81 keywords that formed three clusters (red, green, and blue). To present a clean map, VOSviewer thesaurus files were prepared to standardize terms and exclude generic or out-of-scope terms. In the keyword maps, for example, coronavirus-related terms, generic terms (e.g., health survey, diseases, humans, viral disease), and type of publication or study (e.g., article, case report, editorial) were excluded. Further, commonly cited keywords which are often linked with COVID-19, including ‘pneumonia’, ‘pandemic’, ‘epidemic’, and ‘outbreak’ were excluded to better reflect clarity in the visualization.
-
The lines connecting the circles represent the co-occurring keywords. The distance between two keywords approximates how strongly the words are related based on the number of their co-occurrences (i.e., the more publications in which two keywords co-occur, the stronger the relation between them). Thus, the strongly related words appear closer together on the map.
-
Each distinct color represents a cluster of keywords that are strongly related to each other.
-
The largest cluster (red) were mostly related to public health measures, disease epidemiology, and health system capacity. The keywords, ‘refugee’, ‘migrant’, and ‘vulnerable population’ are found in this cluster. The map revealed countries and region associated in these cluster include: ‘United States’, ‘Italy’, ‘India’, ‘Europe’, and ‘United Kingdom’. The next cluster (green) were mainly related to population characteristics and diagnostic procedures. In the blue cluster, the term ‘travel’, ‘transmission’, and ‘China’ were strongly linked, this indicates the number of publications in which these keywords co-occurred. Majority of the associated terms in these clusters were related to public health control measures and disease epidemiology.
-
In terms of specific research themes, the map was dominated by keywords related to disease epidemiology (i.e., ‘mortality’, ‘infection risk, risk factor’, ‘infection rate’, etc.) and public health measures (i.e., ‘quarantine’, ‘infection control’, ‘social distancing’, ‘disease control’, ‘lockdown’, ‘isolation’, etc.). These were followed by keywords related to health system capacity (i.e., ‘health service’, ‘health policy’, ‘health personnel’, ‘health care access’, etc.), diagnostic procedures (i.e., ‘PCR’, ‘tomography’, and ‘isolation and purification’, etc.), and clinical management and symptoms (i.e., ‘practice guidelines’, ‘fever’, ‘cough’, ‘dyspnea’, etc.). A few keywords were related to policy and economics, and migrant specific groups (i.e., ‘migrant’ and ‘refugee’). There were no keywords on candidate therapeutics and vaccine.
Note: See the full paper for more detailed findings, including the Methodology and Limitations of this analysis.